
AuDHD Diagnosis, Part 2: Formal Diagnosis
This 3-part series is a deep dive into the increasingly relevant—and often contentious—topic of formal vs. self-diagnosis in adults with autism and/or ADHD.
Part 2 Overview: Formal Diagnosis
Introduction
Pros and Cons
Why Seek a Formal Diagnosis of Autism &/or ADHD?
Why NOT Seek a Formal Diagnosis?
Formal Diagnosis: A Flawed Framework
Intro to the DSM-5
Who Does the DSM-5 Leave Behind?
A Neurodivergent-Informed Approach
Diagnostic Tool: The SAAT
Reflections
Introduction
In this post, we’re going to talk about formal diagnosis—that is, seeking out a professional that can diagnose you with autism and/or ADHD. We’ll start off with the basics—some of the most common reasons why or why not people decide to seek a formal diagnosis of autism and/or ADHD. After that, we’ll go down a rabbit hole of deconstructing the systemic bias and discrimination in autism/ADHD formal diagnosis! (If that isn’t the most social work sentence I’ve ever typed…).
Disclaimer: Please note that there is no right or wrong option when seeking a diagnosis, as long as it feels like the right decision for you. I am just one neurodivergent voice in the community, and this series is intended to be informative and critical of the current realities of diagnosis, particularly formal diagnosis—not to dissuade from this option. Every neurodivergent journey, no matter the path, is worthy of recognition and validation. :)
Pros and Cons
Why Seek a Formal Diagnosis of Autism &/or ADHD?
Here are some common reasons why people pursue a formal diagnosis of autism and/or ADHD:
Accommodations at school or work
Many employers/institutions require records of an official diagnosis and/or a doctor’s note of recommendation for accommodations.
Meds
This is why I sought my ADHD diagnosis: I wanted to be prescribed stimulant medication to help me focus during university. I am not advocating for or against managing ADHD with meds; this is just another tool that can be helpful for some, and a common reason for seeking an ADHD diagnosis.
To qualify for social supports
For example, Canada has a disability tax credit that would require documentation of diagnosis.
Simply wanting to: Any reason is valid!
Any other reasons, from needing certainty and self-understanding to demonstrating validity to others, justifies pursuing a formal diagnosis of autism, ADHD, or both.
Why NOT Seek a Formal Diagnosis?
Stigma can manifest as additional barriers when someone gets formally diagnosed, particularly with autism. Here are some potential complications, rooted in systemic stigma, that can arise specifically from being associated with a formal label:
Healthcare disparities
When a healthcare provider sees a diagnosis of autism on your file, it can impact the quality of care you receive. It’s common for autistic folks to experience discrimination in the medical system, from feeling unheard to being flat-out denied healthcare (Johnson, 2022).
Legal injustices
I remember a story once told to me by an autistic peer; she had gotten into a fender bender and went to the police station to report it. Her delayed processing, combined with adjusting to an unfamiliar space, was not compatible with the interrogation-like communication of the officer she was reporting to. She was accused of lying and ended up having a meltdown at the station—even then, she received little warmth, patience, or guidance through the process. I am assuming the officer did not know she had an autism diagnosis (not defending their behaviour), but this story paints a good picture of discrimination in the justice system at an everyday level.
An official autism diagnosis can come with its own issues in the legal system, however. For instance, autistic parents can be denied custody of their children, and autistic adults are at an increased risk of being forced under guardianships without consideration of less-restrictive options (Autism Spectrum News, 2023).
Formal Diagnosis: A Flawed Framework
If you live in North America and seek a formal diagnosis of autism and/or ADHD, the psychologist, psychiatrist, or other diagnosing professional will likely follow criteria outlined by the DSM-5-TR. This diagnostic tool has been controversial in the neurodivergent community in terms of how it represents autism and ADHD.
Intro to the DSM-5
DSM = The Diagnostic and Statistical Manual of Mental Disorders
5-TR = Fifth edition, text-revision. The DSM-5 was published in 2013 and the DSM-5-TR was published in 2022. Because the text-revision is not a new edition of the book, it is common to omit the “TR” in casual discussion, as I do in this post.
Author: American Psychiatric Association (APA)
Purpose: “…to diagnose and classify mental disorders with concise and explicit criteria intended to facilitate an objective assessment of symptom presentations in a variety of clinical settings” (APA, n.d.).
Autism Spectrum Disorder (ASD) and ADHD are classified in the DSM-5 under Neurodevelopmental Disorders. Since 2013, a person can be diagnosed with both; however, there is no diagnosis for AuDHD—this term was coined by its community.
Check out the DSM-5’s official diagnostic criteria for ASD and ADHD.
Who Does the DSM-5 Leave Behind?
“Current tools for identifying autism are critiqued for their lack of specificity and sensitivity, especially in autistic people who are older, have higher verbal ability or significant compensatory skills, and are not cisgender boys. ”
Ratto et al. (2023) is a team led by two autistic researchers; their research is rooted in the notion that diagnostic tools for autism should be informed by autistic people, rather than observations of non-autistic clinicians. They identified three areas* in which the DSM-5 fails to be an inclusive diagnostic tool for autism:
*Ratto et al.’s (2023) research focuses exclusively on autism, but I argue that all three areas can also pertain to the DSM-5’s diagnostic criteria for ADHD.
#1. The APA has always researched autism & ADHD in young, white, presumably cis boys from affluent backgrounds, who display “obvious”, outward signs.
The DSM-5 is still based on research that mostly looked at young, white, cis boys, which reinforces a narrow idea of what autism and ADHD looks like. This means people outside this group—adults, women, girls, racialized and gender-diverse folks—often get overlooked when seeking a diagnosis because presentations of neurodivergence vary among these groups. As well, many cis women and gender-diverse autistic people have developed strong masking traits, which can make their autism harder to spot during assessments (McQuaid, Lee, & Wallace, 2022).
Many professionals that are qualified to provide formal diagnosis are still biased towards the stereotyped, outward presentation of autism and/or ADHD, which makes sense given the widespread use of limited diagnostic tools. My GP exemplified this bias in the medical system—being an overachiever in school can be quite common among girls with ADHD.
This is not to say that neurodivergent-informed professionals don’t exist. However, one of the most financially accessible means of formal diagnosis in Canada requires a psychiatrist, who will most likely use the DSM-5 to provide a diagnosis. While formal diagnosis may be the right answer for many, it runs the risk of being an invalidating experience, particularly for people that aren’t young, white boys.
See Resources below for more information on racial and gender bias in autism/ADHD diagnosis.
#2. Deficits-based model
The DSM-5 frames autism & ADHD based on their shortcomings. The criteria was developed in the context that their is a “normal”, and that autistic/ADHD people fail to meet that standard. As Ratto et al. (2023) describe, the DSM-5’s deficits-based model “posits the non-autistic experience as the default” (p. 94).
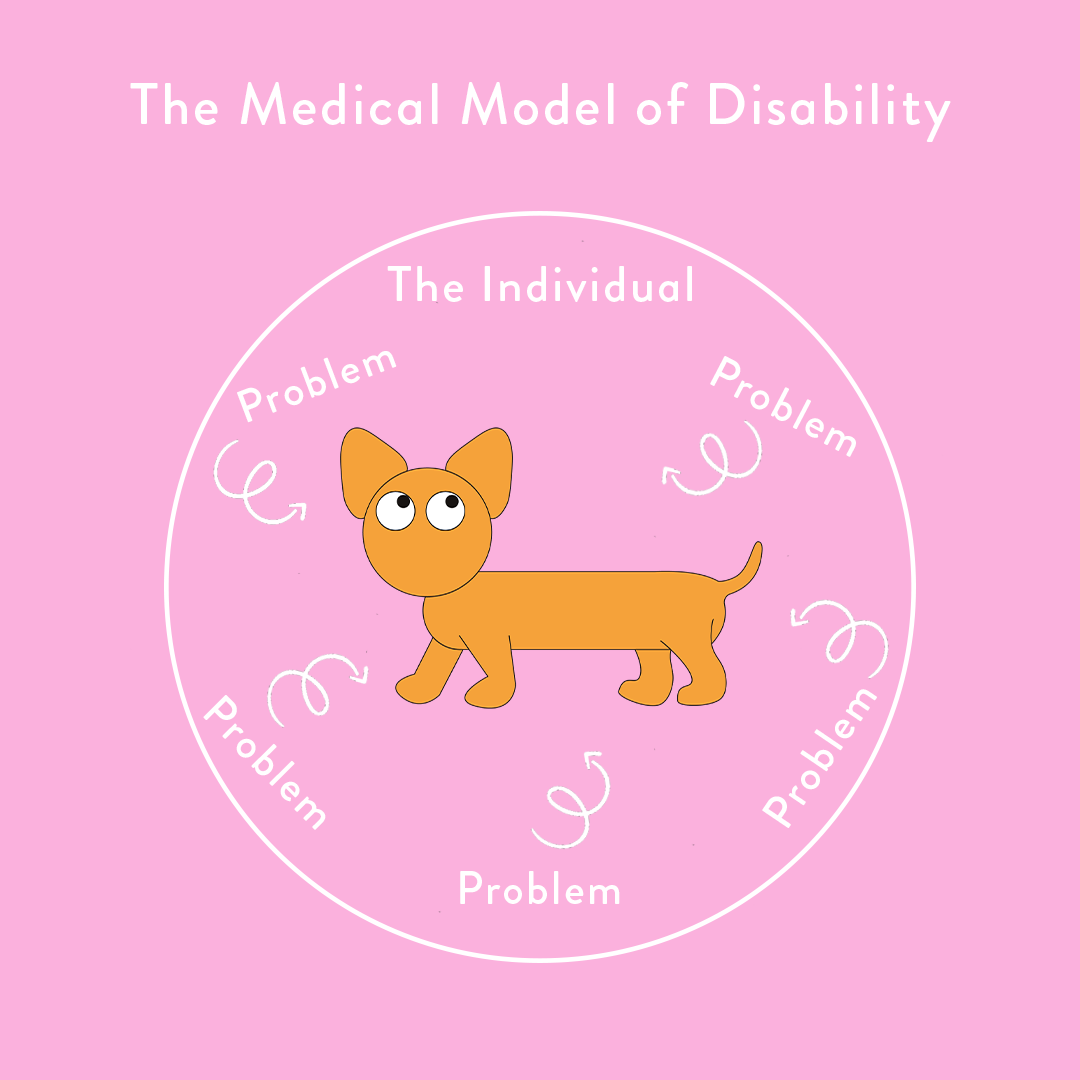
Another word for this model is the medical model of disability.
The medical model views disability as a problem with the individual, a deficit that needs to be fixed (Buder & Perry, n.d.). It defines disability based on how “well” an individual participates in everyday society—can they work 5 days a week, and contribute to the economy? Can they drive to work daily on the busy freeway? If not, the medical model of disability says the issue lies within the individual for failing to meet these norms.
This model labels these “problems” within the individual as pathologies (ex. labelling autism/ADHD as “disorders”).
Image: (Social Creatures, n.d.-a)

In contrast, the social model of disability defines disability by context, saying that “people are disabled by barriers in society, not by their impairment or condition” (Scope, n.d.).
Barriers may be physical, such as a lack of wheelchair ramps, or they may be stigma-fueled attitudes and assumptions about disability. Unlike the medical model, it doesn’t define disabilities as deficits, rather, differences that should be taken into account in society and when designing both social and physical environments.
It’s important to note that it’s up to the individual on how they see/define their disability, whether it’s through the lens of the medical model or the social model, or both.
Image: (Social Creatures, n.d.-b)
“Ultimately, the social model of disability proposes that a disability is only disabling when it prevents someone from doing what they want or need to do. ”
Some reflections that came up for me while writing this section: Living in Alberta, it’s the norm to drive everywhere. I’ve lived in both Edmonton and Calgary as a non-driving adult; I can attest to these cities not being overly convenient to navigate on public transit, unless you strike gold with your location and destination—a clear example of society’s inherent ableism. Before I got my driver’s license, most people—and I am not exaggerating—would gasp, “Really?! Why not?!” when I shared that as a twenty-something, I didn’t drive. This showed me the powerful influence norms have over us, and how easy it is to not question them until they directly impact us. To me, not driving was a no-brainer, and I was always confused (and often ashamed) at the shock of others when they learned this about me. But, if I didn’t struggle so much with the sensory experience (and financial impacts) of driving, who’s to say that I wouldn’t have had the same reaction if someone told me they didn’t drive?
….
Society’s deficit-focused perspective also neglects to recognize the unique strengths of autistic individuals, such as enhanced visual processing, memory, honesty, empathy, creativity, and meticulous attention to detail—some of these traits have shown to be particularly pronounced in autistic people compared to neurotypicals (Ratto et al., 2023). However, when these aspects of the autistic experience are inadequately captured by mainstream diagnostic tools, it’s no surprise that autism is highly stigmatized and misunderstood.
#3. Does not account for internal autistic experiences
An autism assessment, as per the DSM-5, involves the following: Collecting evidence of observable impairments through a review of developmental history and direct behavioral assessments with the individual (Ratto et al., 2023).
Have you ever sought professional help for a mental health concern? Were you given a questionnaire to fill out beforehand? Personally, I have filled out doctor-administered self-screening tools for anxiety, depression, and PTSD. It seems that we trust the internal experiences of people seeking these types of diagnoses, using self-reporting as a valid insight into whether or not someone qualifies for a diagnosis.
But when it comes to seeking a formal autism diagnosis, the process suggests that an autistic person’s inner experiences aren’t trusted—or even considered—as valid evidence.
And, importantly, this decision is not supported or rationalized by any evidence that self-report tools are less accurate in this population (Ratto et al., 2023).
The diagnostic process of autism reflects the belief that all autistic people have limited abilities around introspection and self-awareness. This is nothing more than an assumption—it’s false.
A Neurodivergent-Informed Approach
What if the autistic community created a diagnostic tool?
Diagnostic Tool: The SAAT
Ratto et al. (2023) sought to develop a diagnostic criteria for autism that addressed all three gaps in the DSM-5 detailed above. In collaboration with a diverse autistic expert panel, the Self-Assessment of Autistic Traits (SAAT) was created. The SAAT consists of a series of questions to be answered by the individual; they will score each question as “not true”, “in the middle”, or “completely true”.
Here’s a comparison between some of the diagnostic criteria of the DSM-5 and the SAAT:
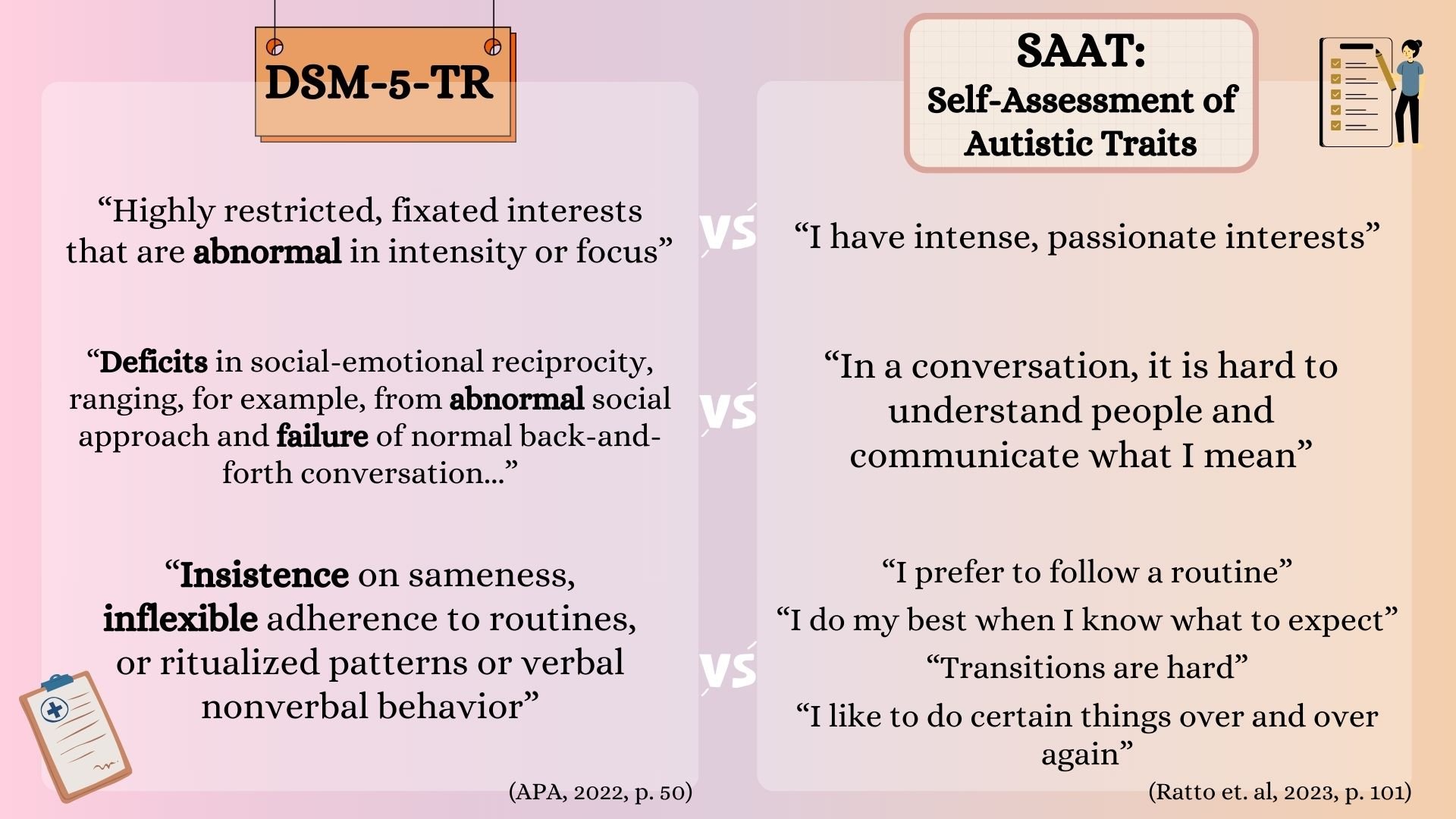
What connotations do the bolded words carry?
Comparing the criteria side by side was eye-opening for me in terms of understanding the deficits-based lens of the DSM-5. I find the language in the SAAT to be neutral yet validating of common autistic struggles. I also like how the criteria is centered from the perspective of the individual, not from a professional’s objective assessment of the person. It makes more sense to me—if autism is a brain difference, then why are only external manifestations considered, and not even from the perspective of the person experiencing them?
Reflections
Writing this post left me with more questions than answers—the aftermath of a successful rabbit hole spiral, in my opinion :). Here are some reflection questions that I will be pondering as we move towards redefining and expanding our understanding of neurodivergence:
How does the language in the DSM-5 contribute societal stigma of autism/ADHD?
How do you think societal attitudes and assumptions towards autism would change if the SAAT took place of the DSM-5? Do you think they’d change at all?
What would society—or even your everyday environment—look if it operated through the social model of disability?
Do you think a formal diagnosis should be required to access accommodations (at work, school, etc.)? Why or why not?
“INTERSECTIONALITY “We do not live single issue lives” –Audre Lorde. Ableism, coupled with white supremacy, supported by capitalism, underscored by heteropatriarchy, has rendered the vast majority of the world “invalid.””
Contributed by Riley, BSW practicum student.
Up Next…
AuDHD Diagnosis, Part 3: Self-Diagnosis
For AuDHD education, support, and resources, check out @riley.unscriptedco on Instagram
Resources
-
-
References:
American Psychiatric Association. (n.d.). What is ADHD?https://www.psychiatry.org/patients-families/adhd/what-is-adhd
Autism Speaks. (n.d.). Autism diagnostic criteria: DSM-5. https://www.autismspeaks.org/autism-diagnostic-criteria-dsm-5
Autism Spectrum News. (2023, July 5). Rights and challenges for autistic people with communication disabilities in the legal system. https://autismspectrumnews.org/rights-and-challenges-for-autistic-people-with-communication-disabilities-in-the-legal-system/
Buder, S., & Perry, R. (n.d.) The social model of disability explained. Social Creatures. https://www.thesocialcreatures.org/thecreaturetimes/the-social-model-of-disability
Canada Revenue Agency. (n.d.). About the disability tax credit (DTC). Government of Canada. https://www.canada.ca/en/revenue-agency/services/tax/individuals/segments/tax-credits-deductions-persons-disabilities/disability-tax-credit/about-dtc.html
Johnson, D. (2022, April 13). Injustices towards people with Autism Spectrum Disorder in health care. Markkula Center for Applied Ethics. https://www.scu.edu/ethics/healthcare-ethics-blog/injustices-towards-people-with-autism-spectrum-disorder-in-health-care/
McQuaid, G. A., Lee, N. R., & Wallace, G. L. (2022). Camouflaging in autism spectrum disorder: Examining the roles of sex, gender identity, and diagnostic timing. Autism, 26(2), 552-559. doi: 10.1177/13623613211042131
Ratto, A. B., Bascom, J., daVanport, S., Strang, J. F., Anthony, L. G., Verbalis, A., Pugliese, C., Nadwodny, N., Brown, L. X. Z., Cruz, M., Hector, B. L., Kapp, S. K., Giwa Onaiwu, M., Raymaker, D. M., Robison, J. E., Stewart, C., Stone, R., Whetsell, E., Pelphrey, K., & Kenworthy, L. (2023). Centering the inner experience of autism: Development of the self-assessment of autistic traits. Autism in Adulthood, 5(1), 93-105. DOI: 10.1089/aut.2021.0099
Scope. (n.d.). The social model of disability. https://www.scope.org.uk/social-model-of-disability
Sins Invalid. (2021, March 24). 10 principles of disability justice [Video]. YouTube. ASL 10 Principles of Disability Justice - YouTube
Social Creatures (n.d.-a). The medical model of disability [Infographic]. https://www.thesocialcreatures.org/thecreaturetimes/the-social-model-of-disability
Social Creatures (n.d.-b). The social model of disability [Infographic]. https://www.thesocialcreatures.org/thecreaturetimes/the-social-model-of-disability
The Spectrum Clinic (n.d.). ADHD presentation in girls and females.https://www.thespectrumclinic.com/post/adhd-presentation-in-girls-and-females#:~:text=Compensatory%20Behaviours%3A%20Girls%20often%20develop,the%20struggles%20they%20are%20facing.